Although I discussed similar issues in a prior post on US health outcomes, I recently stumbled across a JAMA article authored by several CDC researchers (h/t @bswud) which points out that drug poisonings, fire-arm homicides, and motor vehicle accidents can directly explain a large part of the US life expectancy gap with several major comparison countries. By “directly” I mean that which can be mathematically estimated through the actual causes of death instead of its statistical association with life expectancy more broadly. The actual causal effect from statistical estimates are likely to be inflated by other factors that are associated with it (though I personally believe there is still a meaningful signal in the difference between the two estimates insofar as it can act as a proxy for other lifestyle differences as well and that these sorts of differences are far more important than modest differences in how health care is provisioned between different developed countries at present)
In 2012, the all-cause, age-adjusted death rate per 100 000 population was 865.1 among US men vs 772.0 among men in the comparison countries (Table 1), and 624.7 among US women and 494.3 among women in the comparison countries. Men in the comparison countries had a life expectancy advantage of 2.2 years over US men (78.6 years vs 76.4 years), as did women (83.4 years vs 81.2 years). The injury causes of death accounted for 48% (1.02 years) of the life expectancy gap among men. Firearm-related injuries accounted for 21% of the gap, drug poisonings 14%, and MVT crashes 13%. Among women, these causes accounted for 19% (0.42 years) of the gap, with 4% from firearm-related injuries, 9% from drug poisonings, and 6% from MVT crashes. The 3 injury causes accounted for 6% of deaths among US men and 3% among US women.
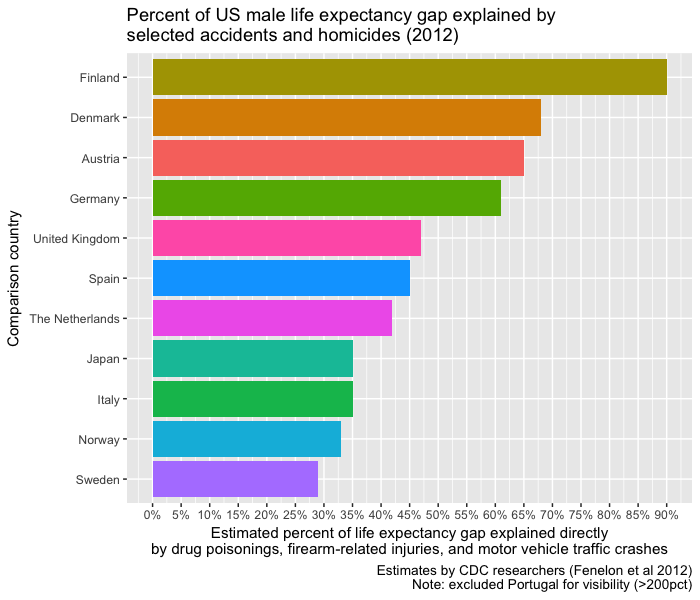
The US death rates from injuries exceeded those in each comparison country (Table 2). Among men, these injuries accounted for more than 50% of the life expectancy gap with Austria, Denmark, Finland, Germany, and Portugal. Among women, they accounted for more than 30% of the gap with Denmark, the Netherlands, and the United Kingdom. The country-specific comparisons depend partly on the actual size of the gap in life expectancy between the United States and each country. For example, men in Portugal have lower injury mortality than US men, but a small life expectancy advantage, which results in the 3 injury causes accounting for more than 100% of the gap.
They didn’t provide any visualizations so I thought I’d share some using their estimates.