Previously I demonstrated that actual individual consumption (AIC) is a superior predictor of national health expenditures (NHE) and largely explains high health spending in the United States. Towards this point it is instructive to show that not only are health expenditures generally coordinated with AIC, but that all other major categories of expenditure are too, i.e., at given level of real consumption per capita all countries will tend to allocate their consumption quite similarly.
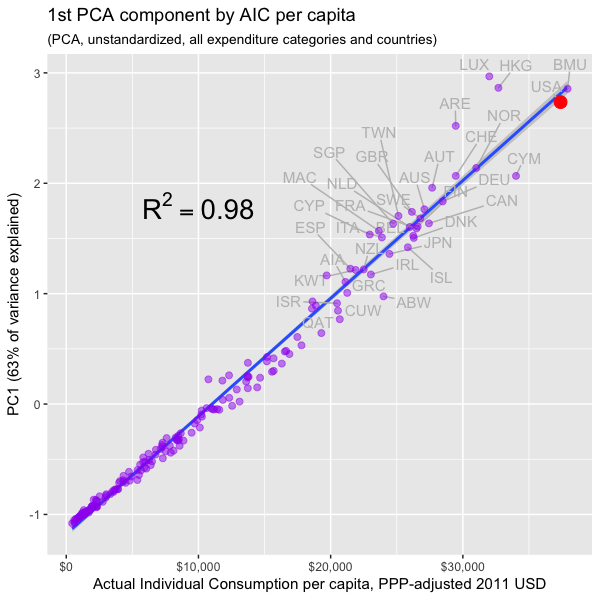
In this post I make extensive use of Principal Components Analysis (PCA) and related dimension reduction techniques to better characterize consumption patterns across several major categories of consumption in both the spatial and temporal dimensions. I find that there is a latent factor that explains the great majority of the variance in consumption, that it is exceptionally well correlated with AIC, and that GDP has essentially zero incremental validity once we have accounted for AIC for practical purposes. I also show that this factor holds up well to price adjustment for each consumption category and correlates similarly with AIC within the OECD.
Although my interest here is (was) largely in verifying my prior analysis as it pertains to health expenditures, i.e., that AIC is real, meaningful, and the measure we probably ought to prefer when discussing the efficacy of cost containment regimes, my analysis has broader implications. For instance, it provides evidence (albeit in a roundabout fashion) that argues rather strongly against Scott Alexander’s widely cited post on cost disease, i.e., if health, education, construction, and so were truly uniquely expensive in the United States, the United States ought to stick out like a sore thumb in PCA and the like. Instead what we found is that the US consumption patterns track well with its high overall level of real consumption (AIC). Moreover, anticipating the argument that perhaps cost disease is simply well correlated with AIC, when we adjust for category specific price levels (i.e., “volumes”) we find PPP-adjusted AIC holds up very well in explaining the variance in the actual volumes consumed overall and that the US is, again, well on trend (which suggests actual apples-to-apples differences in cost are not the problem and actual increase in the quantity and quality of goods & services consumed in these categories drive most of the variance).
Continue reading